The Diaphragm-Psoas Connection
The Daily Bandha
Sankalpa, Visualization and Yoga: The Diaphragm-Psoas Connection
The Sanskrit word “Sankalpa” has been interpreted to mean a “resolution” or “intention”, usually in association with the practice of Yoga Nidra. According to Swami Saraswati, “sankalpa has the potential to release tremendous power by clearly defining and focusing on a chosen goal.” The focus of this blog post is to illustrate the subtle, yet powerful myofascial connections between the diaphragm and iliopsoas muscle all the way down to the feet in Triangle pose. Understanding and visualizing these connections in Trikonasana will enable you to do the same in other poses.
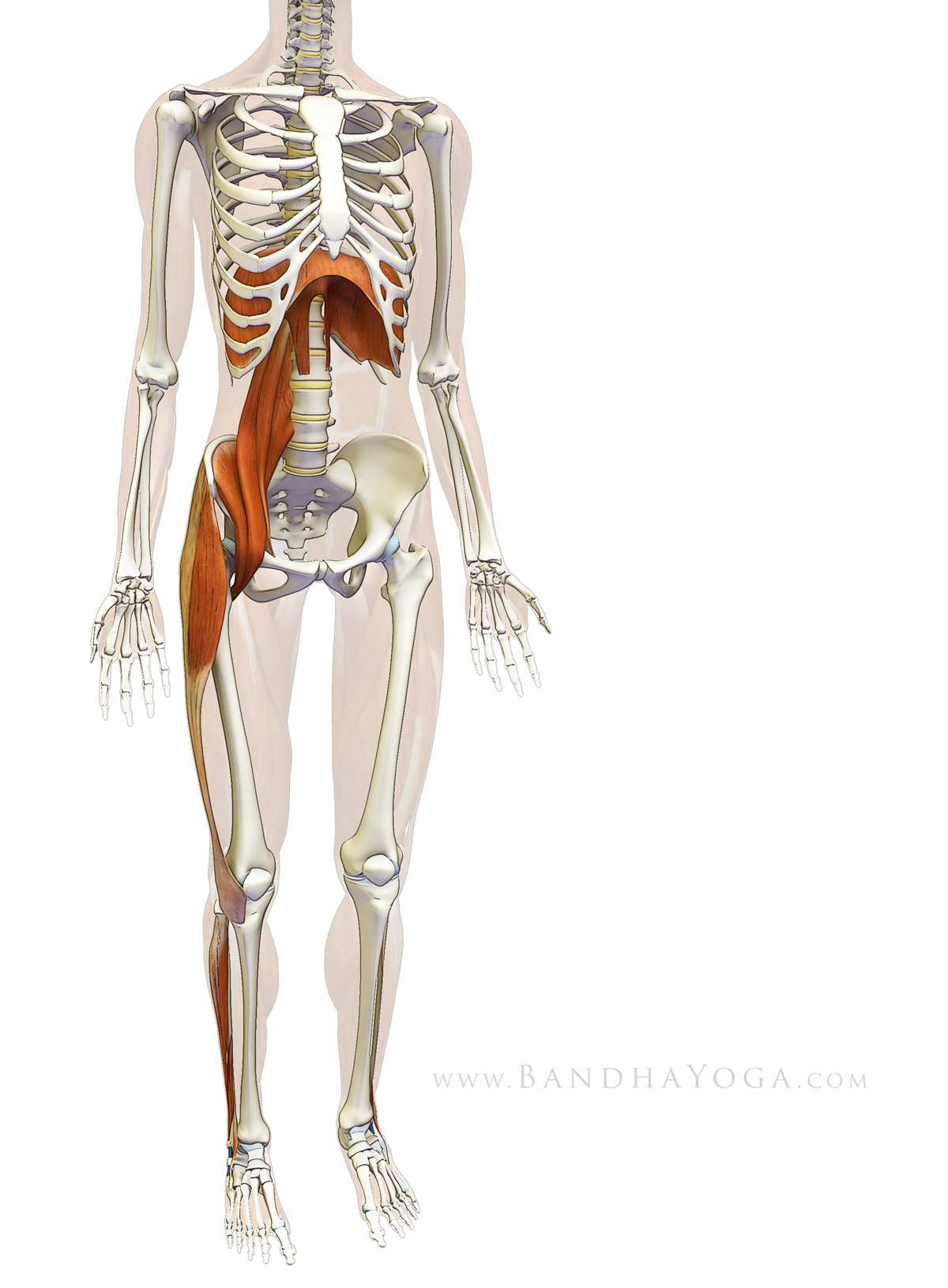 |
| Figure 1: Myofascial connections between the diaphragm, psoas and lower extremity. |
The diaphragm, as we all know, is the central muscle of breathing. It operates mostly unconsciously, though we can consciously influence its rate and depth of contraction. As the central muscle of breathing the diaphragm is inextricably linked to our life force and thus, our emotions and energetic body. Practicing yoga asanas influences the diaphragm in subtle ways, particularly through its connection to the psoas muscle. In fact, every pose has a slightly different effect on the diaphragm, and thus on its energetic connections.
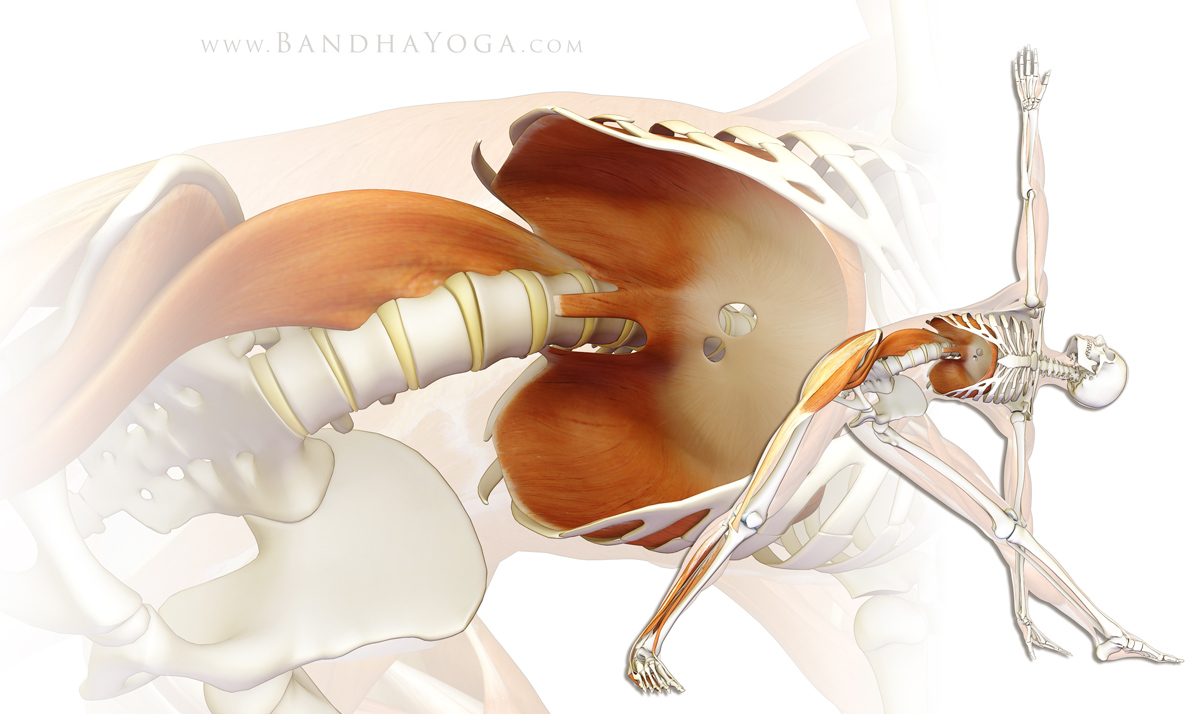 |
| Figure 2: Myofascial connections between the diaphragm, psoas and lower extremity in Trikonasana. |
Visualization is a powerful tool you can use to access these connections. So, before we go on to the details of anatomy and biomechanics, spend a few relaxed moments looking at figures 1 and 2, which illustrate these myofascial connections. Look at the images and then picture the connections within your body (click on the image for a larger view). Repeat this exercise two or three times, devoting five or ten seconds to each visualization. Note how you can feel the connections within yourself. Please complete this process before proceeding with the details of anatomy and biomechanics.
And, here’s the anatomy…
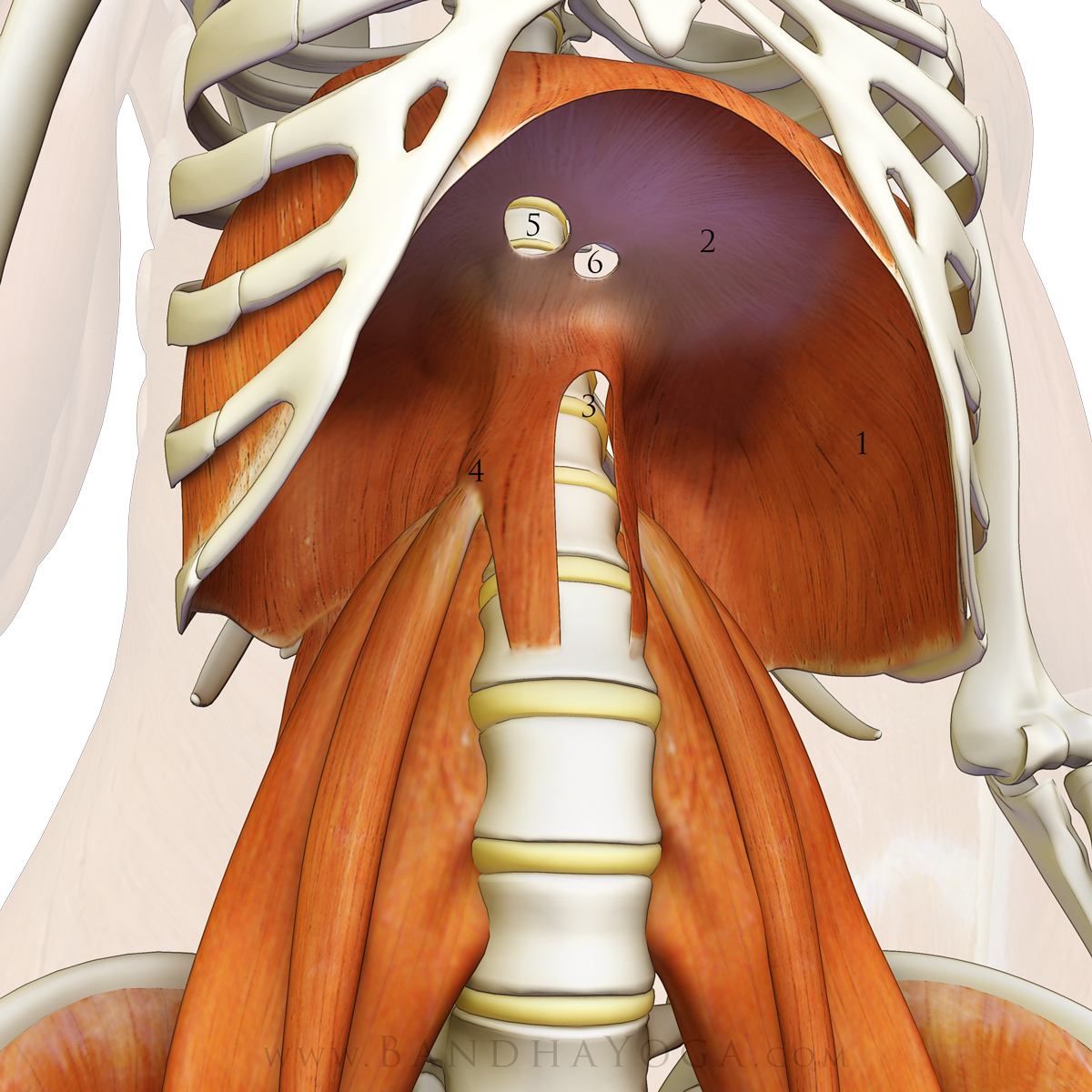
The thoracic diaphragm is a dome shaped muscle that separates the chest and abdominal cavities. The contractile part of this muscle is located peripherally, inserting onto a central tendon (that is not connected to a bone). The origins of the muscle are divided into costal and lumbar portions. The “costal” portion originates from the inner surface of ribs seven through twelve. The “lumbar” portion has both medial (closer to the midline) and lateral (further from the midline) aspects. The medial aspects of the diaphragm arise from the front of the first three lumbar vertebrae (L1-L3). The lateral aspects arise from three tendinous arches. The first tendinous arch is associated with the abdominal aorta, and the second and third with the psoas major and quadratus lumborum muscles respectively. Figure 3 illustrates these structures.
 |
| Figure 3: The diaphragm-psoas connection. 1) diaphragm 2) diaphragm tendon 3) aortic aperture 4) psoas arcade 5) vena caval aperture 6) esophageal aperture |
{kind=link}
Engaging the diaphragm with the glottis open expands the ribcage and produces a pressure gradient by lowering intrathoracic pressure. The negative inspiratory pressure causes air to be drawn into the lungs, thus equalizing the gradient. These fluctuating pressure gradients also facilitate blood flow, particularly venous return to the heart.
Conversely, contracting the diaphragm after exhalation with the glottis closed (as in Nauli) also produces a pressure gradient. In this case the negative inspiratory pressure draws the abdominal contents upwards (and the abdomen in). Engaging the diaphragm on exhalation with the glottis closed is a form of eccentric (or isometric contraction), whereby a muscle is engaged in its lengthened state, but does not shorten.
Engaging the abdominals during exhalation passively stretches the diaphragm by raising the intra-abdominal pressure and lifting the abdominal organs upward against the muscle. Note that engaging the abdominals on exhalation also tensions the thoraco-lumbar fascia, which serves to stabilize the lumbar spine and sacroiliac joint. Click here for more information on this particular connection.
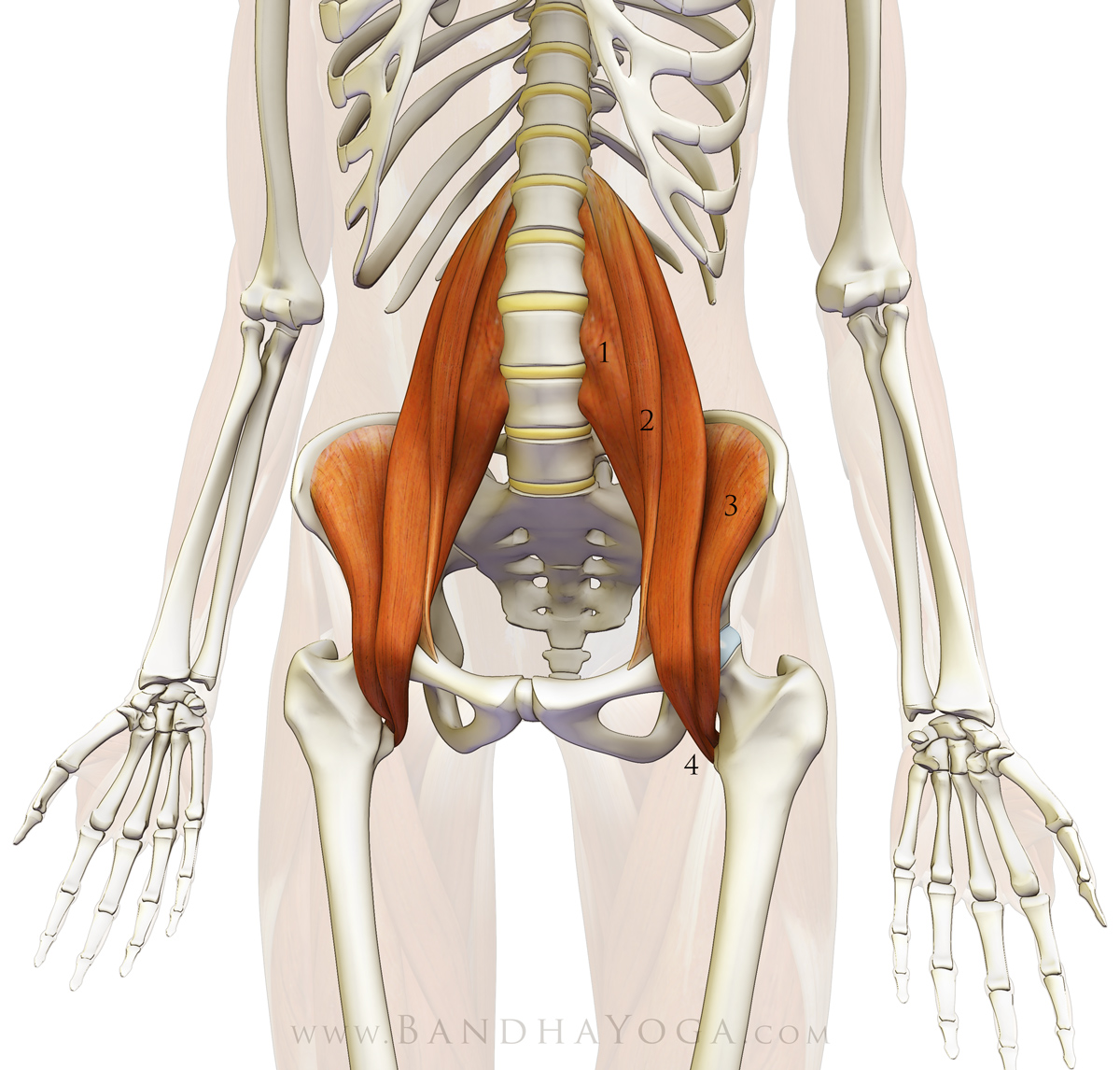
The psoas major muscle originates from the vertebral bodies of T12 and L1 through L4 (lateral surfaces and discs), with a deep layer originating from L1-L5 (costal processes). It combines with the iliacus muscle, which originates from the inside of the ilium (the iliac fossa) to form the iliopsoas muscle. The iliopsoas then runs over the brim of the pelvis to insert onto the lesser trochanter, a knob-like structure on the upper, inside of the femur (thigh bone). The iliopsoas crosses multiple joints and is thus considered a polyarticular muscle. When contracting on one side it can act to flex and externally rotate the femur and/or laterally flex the trunk (as in Trikonasana) or tilt one side of the pelvis forward. When the iliopsoas contracts on both sides it can flex both femurs and the trunk. Bilaterally contracting this muscle lifts the trunk from supine position (lying on the back). Figure 4 illustrates the iliopsoas muscle. Click here for a technique on isolating and awakening this important muscle to use it consciously in yoga poses.
{kind=link}
 |
| Figure 4: The psoas. 1) psoas major 2) psoas minor 3) iliacus 4) iliopsoas (at tendon attachment to the lesser trochanter) |
Now, return to the images illustrating myofascial connection between the diaphragm, the psoas and the lower extremities (figures 1 and 2). Spend a few moments in relaxed visualization of these key structures. Note how your body awareness has deepened in the brief period between now and when you first looked at them. Integrate this process into your daily practice.
Sankalpa and creative visualization are two of the eight components of Yoga Nidra, as described by Swami Satyananda. Though typically performed during the deep relaxation phase of an asana practice, visualization and intent can be worked with during the asanas themselves. Swami Saraswati beautifully describes the process of Sankalpa as a series of stepping-stones that are used to cross a wide river.